Therapy Options
Selecting a Renal Replacement Therapy modality requires careful consideration of many patient and ICU-specific factors.
Acute Renal Replacement Therapy (RRT) takes several forms that are delivered continuously or intermittently.
Traditional Renal Replacement
This is the traditional, prevailing approach based on utilization of RRT when there is little or no residual kidney function.1
Life-Threatening Indications
Dialysis can be used for treatment related to hyperkalemia, acidemia, pulmonary edema or uremic complications.29
Non-Emergency Indications
Renal replacement therapy can be used in non-emergencies for solute control, fluid removal and the correction of acid-base abnormalities.1
Renal Support
This approach is based on the utilization of RRT techniques as an adjunct to enhance kidney function, modify fluid balance, and control solute levels.1
CRRT is the preferred renal replacement therapy by many clinicians.
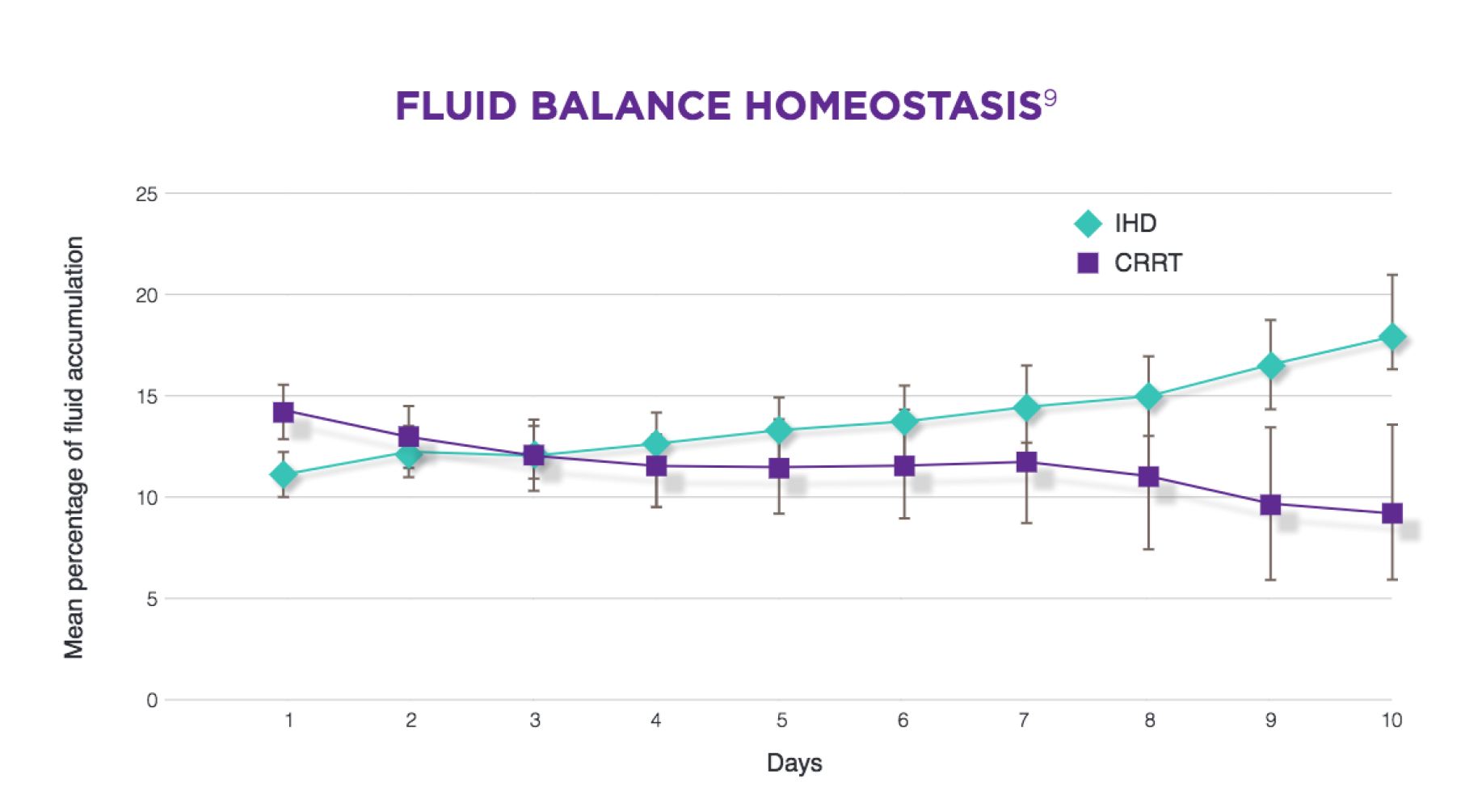
CRRT is RRT that is delivered 24 hours a day. Many clinicians prefer to use CRRT for patients with AKI who are hemodynamically unstable.1 Patients receiving CRRT have had reduced fluid accumulation over time compared with those receiving IHD.1 Fluid overload is independently associated with mortality in patients with AKI.1 CRRT has its own features, risks, and burdens.17 Features relative to CRRT include improved hemodynamic stability and stability of intracranial pressure.18 For example, one study found an increase in brain water content after IHD but no such change following CRRT.17

Intermittent RRT is not continuous by definition.
Its common forms are intermittent hemodialysis (IHD) and prolonged Intermittent Renal Replacement Therapy (PIRRT). Sustained low-efficiency dialysis (SLED) is a form of PIRRT. IHD lasts for 3 to 6 hour sessions done 3 to 7 times per week.20 SLED often runs for 6 to 12 hour sessions, also done 3 to 7 times per week.15 IHD and PIRRT use local water sources to prepare dialysate.15 Water sources must be treated and monitored for quality.23 Intermittent RRT has its own features, risks, and burdens.17 It differs from CRRT by having more infrequent intervals of fluid removal.17 AKI patients on IHD may experience more rapid metabolic and acid-base corrections.17
The selection of renal replacement therapy modality requires careful consideration of many patient and ICU-specific factors.
Fluid overload and hemodynamic instability
CRRT is a preferred RRT by many clinicians for AKI patients who are hemodynamically unstable.1.16
Long-term clinical outcomes and risk of chronic dialysis
Use of CRRT for AKI management has been associated with a lower risk of chronic dialysis compared with IHD.25, 26, 27, 28
Machine delivery and prescription dosing
Unlike IHD, CRRT is run on machines that delivers a more sustained continuous solute removal.29,30
Solution preparation requirements and monitoring
Water treatment and quality testing may contribute to increased monitoring when using solutions prepared on-line for IHD.23, 24
Long-term cumulative costs related to chronic dialysis
The long-term cost of AKI may be lower for patients initially treated with CRRT compared to those treated with IHD.11
Equipment footprint and mobility of water treatment devices
Water treatment equipment may add to the footprint of the IHD system, potentially decreasing treatment mobility and impacting spacing considerations.23,24